




In Remote Patient Monitoring (RPM), Chronic Care Management (CCM), and Remote Therapeutic Monitoring (RTM), clinician time is the most valuable—and the most constrained—resource. We built this project to answer a simple but frustrating question that nearly every clinical team faces: once you’ve handled the critical issues, how do you spend your remaining time in a way that is efficient, compliant, and financially sustainable?
Let me be absolutely clear: this project does not prioritize based on revenue at the expense of patient care. Critical alerts, symptoms, and emergencies are handled first by a separate triage algorithm built for safety, not billing. That’s always the priority. But after those have been handled, we’re left with a queue of lower-urgency patients—all deserving of care, but all competing for limited time.
So the question becomes: which of these patients should I call today? Who gets time? Who gets a reminder? And how do I ensure we’re not wasting effort while still providing meaningful care?
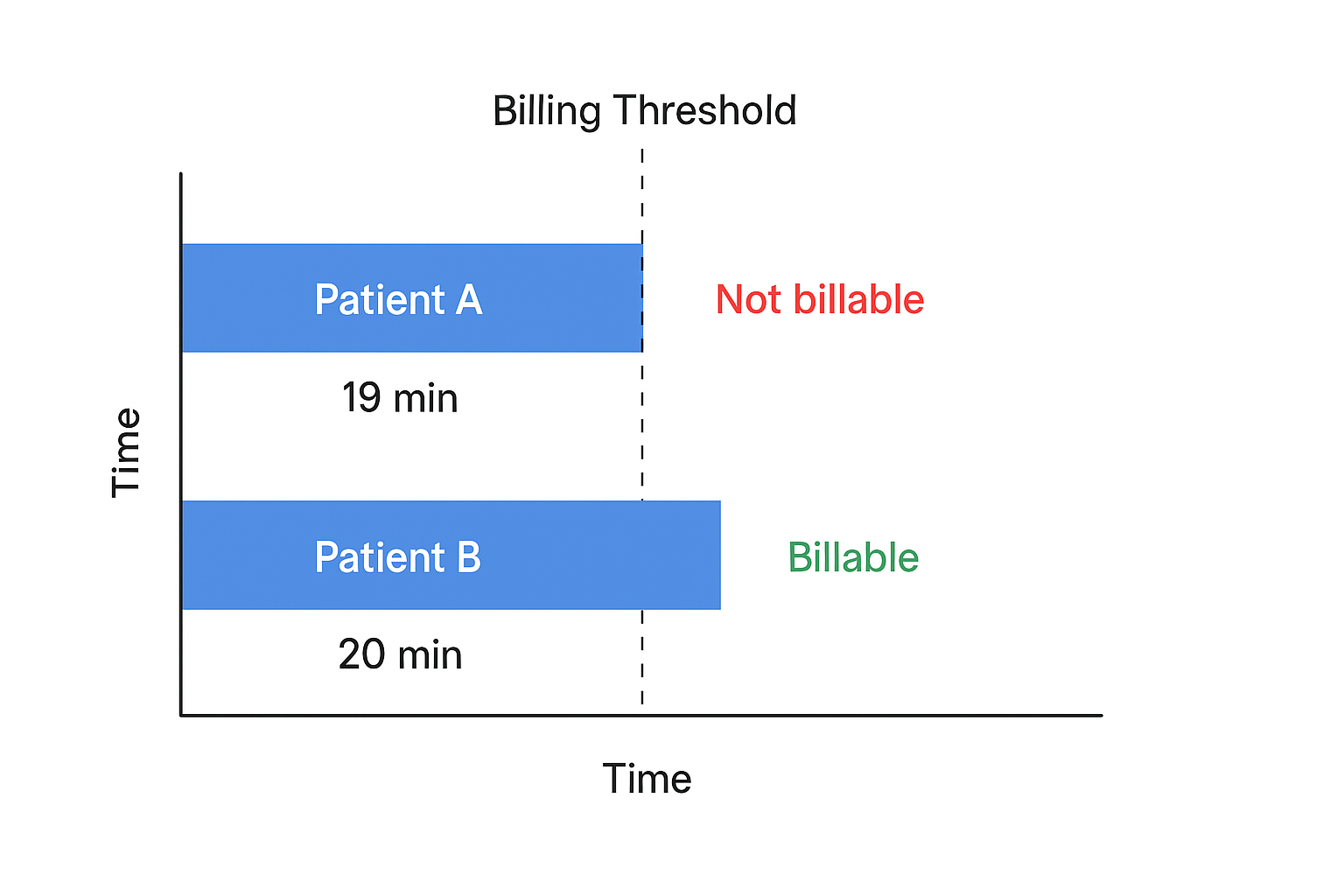
RPM programs are structured around strict time-based billing codes. For example:
But the 20-minute block is absolute. If you log 19 minutes with a patient, you cannot bill. And if you go over 20 but don’t reach 40, you’ve potentially wasted time. So the challenge is aligning care delivery with billing thresholds without treating care delivery as just billing.
Before this system, most clinics made prioritization decisions manually. Clinicians would scan dashboards, try to remember which patients had been contacted recently, and make subjective decisions about who to call next. It was inconsistent, unscalable, and cognitively exhausting.Small clinics especially struggled. They can’t afford optimization staff, complex data teams, or RPA contracts. But they deserve better tools.
To solve this, I modeled the patient prioritization process as a variation of the Multi-Armed Bandit (MAB) problem from decision theory. Each patient is treated as an "arm," with the reward being a successfully billed CPT code.We wanted a system that would:
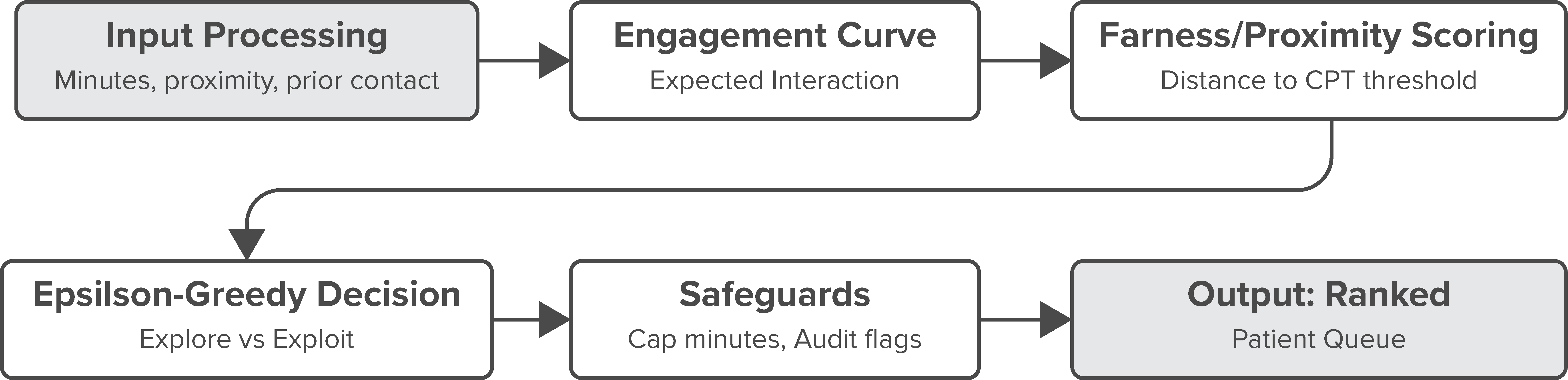
Here’s the breakdown of what happens each day:
One client went from manually auditing 100 patient charts a day to letting the algorithm generate a smart queue—and recovered over $80K in billable time in the first two months.
This isn’t an LLM. This isn’t RPA. This is structured, rules-based AI built for the messiness of real-world clinical operations. It doesn’t hallucinate. It doesn’t guess. It follows rules that are easy to inspect, explain, and justify during an audit.And importantly, it’s built for the clinics that get ignored—the five-provider team in rural Arkansas, the FQHC scraping by on grants, the CCM startup trying to support independent doctors.These clinics don’t have time to waste. This system ensures they don’t.
There is a right way to balance time, care, and compliance—and it starts by respecting clinical judgment while removing the burden of decision-making noise. By using a bandit model with a day-weighted epsilon-greedy strategy, we built a system that adapts over time, works with billing rules, and helps providers do more with less.
We didn’t cut corners. We automated them. And then we used that time to make care better.
This is what it looks like to build practical, transparent AI for healthcare. And it’s already saving providers time, money, and stress—without sacrificing a single patient’s care.
